When surgery is chosen as the first step in treating breast cancer, it can feel overwhelming, but understanding the options and how decisions are made can help you feel more in control.
Here is what a patient and the family members need to know about surgical options, the factors driving the surgeon’s recommendation, and how a tumour board fits into the process.
The Role of the Tumour Board
Before we know what the surgical options are, it is best to understand how a team of doctors from different departments come together to evaluate each patient’s diagnosis and reach a consensus on the right course of treatment.
A Tumour Board is a multidisciplinary team of cancer experts who meet regularly to review and discuss complex patient cases. It typically includes surgical oncologists, medical oncologists, radiation oncologists, radiologists, pathologists, and genetic counsellors, and, in some cases, even anesthesiologists.

When surgery is being planned, the Tumour Board plays a vital role by:
- Providing a Collective Second Opinion: Instead of relying on just one doctor’s perspective, the patient benefits from a consensus of multiple specialities looking at the same data.
- Reviewing Pathology and Imaging: The pathologists and radiologists re-verify the exact stage, grade, hormone receptor status (ER/PR), and HER2 status to ensure the diagnosis is 100% accurate before anyone picks up a scalpel.
- Sequencing the Treatment: They determine whether surgery should truly be the first step. For instance, they might debate whether neoadjuvant therapy (chemotherapy or hormone therapy before surgery) might shrink a large tumour enough to allow for a lumpectomy instead of a mastectomy.
- Ensuring Evidence-Based Care: They ensure the proposed surgical plan aligns with the most current international clinical guidelines and clinical trials.
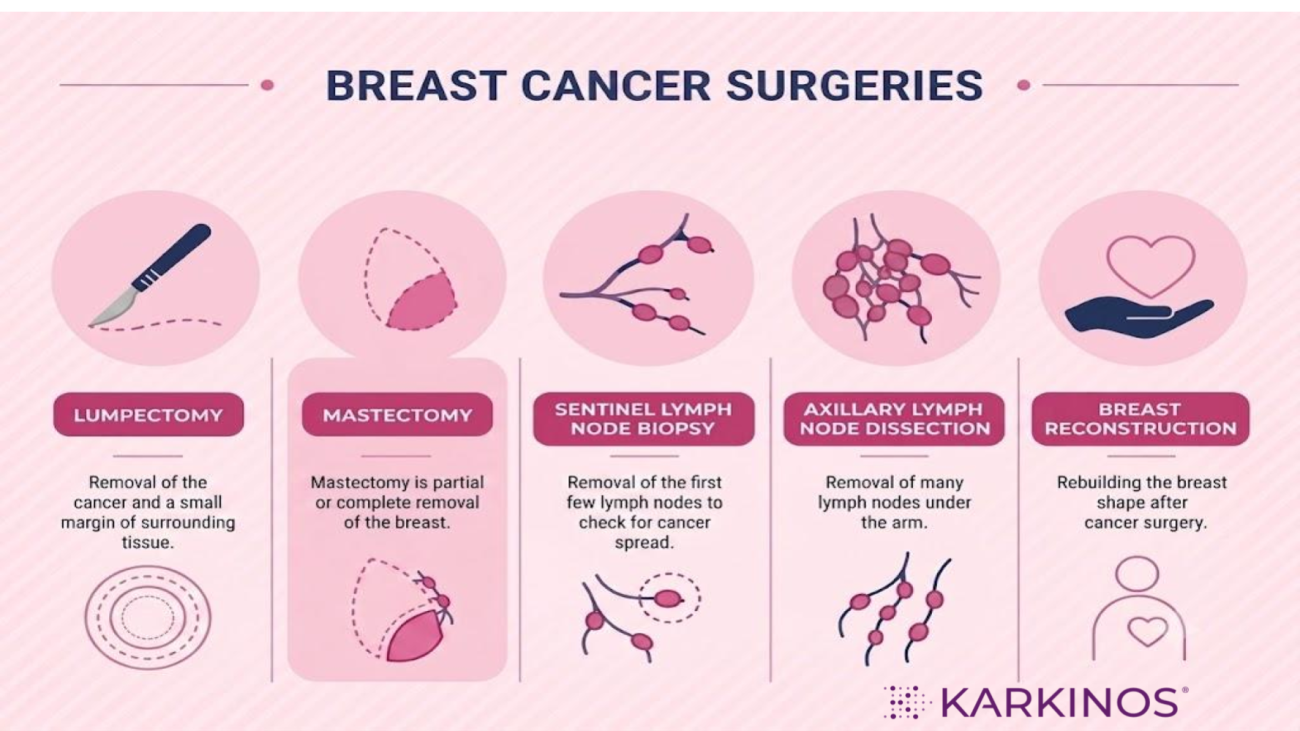
The Main Surgical Options
There are two primary surgical approaches for removing the tumour, often accompanied by an evaluation of the lymph nodes. Before elaborating on the types of surgeries, it is important to understand on what basis the choice of surgery is considered.
A surgeon doesn’t choose an operation at random; the recommendation is tailored to the specific characteristics of the cancer and the patient’s body. Key factors include:
- Tumour Size vs. Breast Size: A large tumour in a small breast might mean a lumpectomy would leave a significant cosmetic deformity, making a mastectomy a better physical option. Conversely, a small tumour in a larger breast is highly suited for breast-conserving surgery.
- Tumour Location and Multi-focality: If there are multiple tumours in different areas (quadrants) of the same breast, a mastectomy is usually required to ensure all the cancer is removed.
- Genetic Factors: Patients with genetic mutations (like BRCA1 or BRCA2) have a very high risk of developing a second breast cancer. They often choose, or are advised, to have a bilateral (double) mastectomy for risk reduction.
- Patient Medical History: If a patient has had prior radiation to that breast or has certain connective tissue diseases (like scleroderma), standard post-lumpectomy radiation may not be safe, making mastectomy the default choice.
- Patient Preference: A patient’s personal comfort level with the risk of recurrence, thoughts on radiation therapy, and desires regarding cosmetic appearance play a massive role.
| Surgery Type | What is Removed? | What is Saved? | Is Radiation Needed After? |
| Lumpectomy | The cancer lump and a small edge of normal tissue. | Most of the breast tissue and the skin. | Yes (Almost always) |
| Mastectomy | Complete or partial removal of the breast tissue. | The chest muscles underneath. | Sometimes (Depends on tumour size and lymph nodes) |
| Lymph Node Biopsy | Only 1 to 3 “sentinel” nodes under the arm. | The remaining lymph nodes. | Depends on the main breast surgery. |
Breast-Conserving Surgery – Lumpectomy
Think of this as a “save as much as possible” approach. The surgeon removes only the tumour and a small border of healthy tissue around it, rather than the whole breast. Simply put, breast conservation surgery (BCS) involves removal of the breast lump with a margin of normal tissue, along with the axillary lymph nodes.
Why the healthy border matters: Removing a thin rim of normal tissue along with the tumour helps make sure no stray cancer cells are left behind at the edges.
Who this is usually suitable for: People with early-stage cancer, especially when the tumour is small compared to the overall size of the breast.
What comes next: This surgery is almost always followed by radiation therapy. Think of the surgery as removing the visible tumour, and the radiation as a follow-up step that mops up any microscopic cancer cells that might still be hiding in the area, lowering the chance of the cancer coming back.
You may also hear this surgery called a partial mastectomy or quadrantectomy. These are simply other names for the same idea: removing the cancer while keeping most of your natural breast tissue intact.
Mastectomy
A mastectomy means removing the entire breast, rather than just the tumour. This may be recommended when the cancer is larger, found in more than one area of the breast, or as a protective step for people at very high genetic risk of developing breast cancer.
Unlike breast-conserving surgery, radiation is not always required afterwards. Whether you need it depends on what is found when the removed tissue is examined under a microscope (the pathology report). Reconstruction to rebuild the breast’s shape is also often possible, either right away or at a later date.
There are a few types of mastectomy, depending on how much tissue is removed:
- Total (Simple) Mastectomy: Removes all the breast tissue, including the nipple and areola. The lymph nodes under the arm are left untouched.
- Modified Radical Mastectomy: Removes all the breast tissue, the thin lining covering the chest muscles, and the lymph nodes under the arm.
- Skin-Sparing or Nipple-Sparing Mastectomy: Removes the breast tissue from underneath while preserving the skin and, in some cases, the nipple. This approach is usually chosen when reconstruction is planned immediately, since preserving the skin envelope yields a more natural-looking result.
Lymph Node Surgery: Checking If Cancer Has Spread
Lymph nodes act like small filtering stations along the body’s drainage system. The ones under your arm filter fluid coming from the breast, so checking them tells your doctors whether any cancer cells have travelled beyond the breast itself.
This is usually done during the same operation as your breast surgery, using one of two approaches:
- Sentinel Lymph Node Biopsy (SLNB): The surgeon removes only the first few lymph nodes that drain the breast, known as the “sentinel” nodes. If these come back cancer-free, it is a good sign, and no further nodes need to be removed. This approach also lowers the risk of side effects like arm swelling (called lymphedema).
- Axillary Lymph Node Dissection (ALND): If cancer is found in the sentinel nodes, or was already known to have spread before surgery, a larger group of nodes (usually somewhere between 10 and 40) is removed from the underarm area for further testing.
Breast Reconstruction
Many people choose to have the shape of the breast rebuilt after a mastectomy. This is entirely a personal choice.
Reconstruction can happen in two ways:
- Immediate reconstruction: Done in the same surgery as the mastectomy.
- Delayed reconstruction: Done months or even years later, once you feel ready.
There are two main techniques used:
- Implant-Based Reconstruction: Uses a silicone or saline implant to recreate the shape of the breast, similar to how implants are used in cosmetic breast surgery.
- Flap (Autologous) Reconstruction: Uses your own tissue, taken from another part of your body such as the abdomen (known as a DIEP or TRAM flap), the back (Latissimus dorsi flap), or the thighs, to rebuild a breast that look and feel more natural since it is your own tissue.
A Note on Oncoplastic Surgery
This is a combined approach where breast-conserving surgery (removing the tumour) and plastic surgery techniques are done together in the same operation. As the surgeon removes the cancer, they also reshape the remaining breast tissue, helping the breast keep a natural appearance afterwards.
A Final Note
These options are not mutually exclusive. For example, someone might have a lumpectomy combined with a sentinel lymph node biopsy and oncoplastic reshaping, all in a single operation. Your surgical team will recommend a combination based on your specific diagnosis, and you are always welcome to ask questions like:
- Why is this particular surgery being recommended for my case?
- Will I need radiation or further treatment afterwards?
- What are my options for reconstruction, and when can I decide?
- What recovery and side effects should I expect?
Medical disclaimer: This article is for general educational purposes only and does not constitute medical advice. Guidelines vary by centre, patient profile, and resource availability. Always consult a qualified oncologist or breast cancer specialist for individual guidance.
Karkinos Healthcare