
In our last article, we examined the specific genes linked to breast cancer and learned that while BRCA1 and BRCA2 are the best-known, several other genes can also play a major role. Now that we know which genes to look for, the next step is understanding how we find them — through genetic testing and counselling.
Genetic testing examines your DNA to detect inherited changes, or pathogenic variants, that increase the likelihood of developing certain cancers. It’s not a crystal ball; it does not predict the future. Instead, it gives your medical team concrete information — for example, whether you carry changes in BRCA1/2, MLH1, TP53, or other genes — that clarifies which cancers you and your blood relatives are at higher risk for.
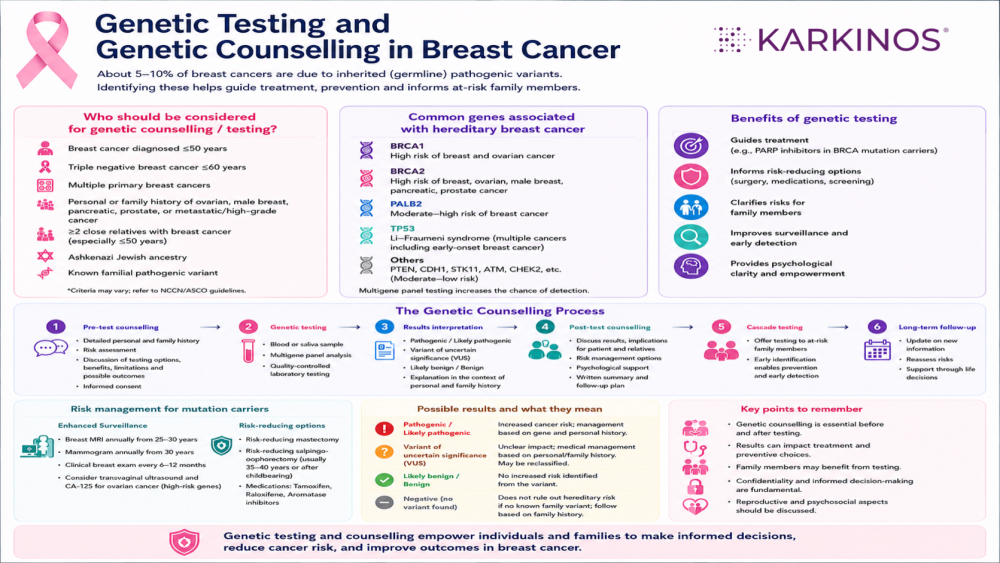
Armed with test results and guidance from genetic counselling, clinicians can tailor screening and prevention strategies to your risk level, such as regular scans, risk-reducing surgery, or targeted therapies. Testing can also inform at-risk family members about the potential need for genetic testing and support the timely implementation of appropriate monitoring, risk-reduction, and preventive strategies.
In the following parts of this blog, you will become familiar with the genetic testing process and how a genetic counsellor assists in the process from pre-test guidance up to planning the right clinical step to prevention or treatment.
Understanding the Genetic Testing Process
For most patients, genetic testing is as straightforward as a routine medical appointment. It does not require surgery, long hospital stays, or lengthy procedures. The process is simple, minimally invasive, and designed to be as convenient as possible. Here is what typically happens, step by step:
- Step 1: The Sample Collection
The test starts with collecting a small sample of your DNA. This is usually done in one of two quick ways: a simple blood draw from your arm, or a saliva swab from the inside of your cheek. - Step 2: Laboratory Analysis
Your sample is sent to a specialised laboratory, where highly trained scientists extract and analyse your DNA. Using advanced genetic testing technologies, they examine specific genes like BRCA1 or BRCA2 to identify genetic changes (variants) that may affect health or increase disease susceptibility. - Step 3: Waiting for Results
It generally takes a few weeks for the laboratory to complete the detailed analysis and send a report back to you or your medical team.
What Does the Test Actually Detect?
The main goal of the test is to look for germline mutations. These are genetic changes that you were born with and that exist in every cell of your body.
In the context of breast cancer, the test detects whether these specific changes have disrupted the genes that normally prevent tumours from growing. Identifying these alterations tells your doctors if your cancer has a genetic cause or if you have a higher baseline risk of developing cancer in the future.
When is a genetic test recommended?
Genetic testing has traditionally been recommended for individuals with certain risk factors, such as a personal or family history of inherited conditions. Because it provides deep, highly specific information about your DNA, healthcare professionals may suggest testing when it could help guide medical care or clarify disease risk.
Deciding when to get tested depends entirely on your personal situation. Doctors generally view genetic testing through two lenses: treatment and prevention.
Everyone can potentially benefit from understanding their genetic makeup, whether for managing an existing condition or planning for future health. For someone already diagnosed with breast cancer, the test helps shape immediate medical decisions. For someone without cancer, it serves as a proactive shield to understand future risks (mainly to prevent hereditary diseases).
Pre-Test and Post-Test Genetic Counselling: Navigating the Process
A genetic test is much more than just a medical procedure; it is a journey that can bring up many questions and emotions. To support you through this, a genetic counsellor works with you at two critical stages: before you take the test, and after your results come back.
Here is how each session helps you find clarity and direction.
1. Pre-Genetic Testing Counselling: Making an Informed Choice
Before you give a blood or saliva sample, you sit down with a genetic counsellor to understand what to expect out of a genetic test. This session is all about preparation and assessment.
- Reviewing Your Family Tree: The counsellor maps out your family’s medical history across generations. They look for patterns of breast, ovarian, or other cancers to see if a genetic link is likely. The counsellor builds a three-generation pedigree. This includes ages at diagnosis for all cancers, bilaterality for breast cancer, site of origin, age at death where relevant, and ethnicity (certain mutations, including BRCA1 c.68_69delAG and c.5266dupC, and BRCA2 c.5946delT, are enriched in specific populations).
- Choosing the Right Test: There is no single genetic test. The counsellor determines whether you need a narrow test (looking only at BRCA1 and BRCA2) or a broader panel test that checks multiple genes.
- Understanding the Benefits and Limitations: The counsellor explains what the test can and cannot tell you, helping set realistic expectations about the results. They discuss the different types of results you may receive, such as positive, negative, or uncertain findings, and what each could mean for your health and medical care.
- Emotional Preparation: The counsellor talks through what a positive or negative result could mean for your mental health and your family, ensuring you feel completely ready to receive the information.
2. Post-Genetic Testing Counselling: Decoding the Results
Once the laboratory finishes analysing your DNA, the genetic counsellor meets with you again. Their job now is to translate complex medical data into a clear, understandable language.
Genetic test results are rarely a simple “yes” or “no.” Your counsellor will explain which of the three possible results you received:
- Positive Result: A harmful mutation was found. The counsellor will gently explain what this means for your current treatment or future risks, and immediately help coordinate next steps with your oncologist.
- Negative Result: No known high-risk mutations were found. The counsellor will explain if this truly lowers your risk, or if you still need close monitoring based on your family history alone.
- Variant of Uncertain Significance (VUS): This means a genetic change has been identified, but the scientific community does not yet have sufficient evidence to determine whether it is associated with disease risk. The counsellor is vital here—they reassure you that a VUS is not a positive result and should not be used to make drastic medical decisions.
Ultimately, post-test counselling turns raw data into an actionable health plan, ensuring you are never left alone to figure out what comes next.
Pre-Test Counselling: What Actually Happens
A pre-test genetic counselling session is more than just a walkthrough of the consent form. It is a structured clinical encounter with three key objectives: establishing prior probability, aligning the test to the clinical question, and preparing the patient for the full range of outcomes. Understanding your genetics helps take away the fear of the unknown. It replaces worry with concrete facts, helping you and your doctors make the best, safest choices for your treatment and your family.
Explaining the test itself
Broad genetic tests such as Whole-Exome and Whole-Genome Sequencing have become standard at most referral centres. Counsellors explain which genes are included (and why), what variants are being looked for (pathogenic, likely pathogenic, variants of uncertain significance), and what a result in each category would and would not mean for clinical management.
Counsellors also explain what these tests can and cannot tell us. A negative result does not completely rule out an inherited condition; it simply means that no disease-causing change was found in the genes that were analysed.
Informed consent: the real content
Genuine informed consent for hereditary cancer testing includes the possibility of a VUS result, the implications for insurability, the potential for results to affect family members who have not consented to testing, and the psychological weight of a positive result. Patients who have considered these dimensions before the test are substantially better positioned to act on results constructively.
Result Categories and What Follows Each
Pathogenic or Likely Pathogenic Variant
A pathogenic or likely pathogenic result confirms the patient carries an inherited mutation in a cancer predisposition gene. The clinical response depends on which gene.
For BRCA1 and BRCA2, evidence-based management options are well-established: enhanced surveillance (annual MRI plus mammography from age 25–30), risk-reducing surgery (bilateral mastectomy, salpingo-oophorectomy), and, in the metastatic or neoadjuvant setting, PARP inhibitor eligibility. For other genes — PALB2, CHEK2, ATM, TP53, PTEN — management is guided by the gene’s associated penetrance and the patient’s personal and family history, and is typically reviewed by a multidisciplinary team.
The post-result counselling session here has a clinical agenda: reviewing next steps and management options, addressing questions about timing of risk-reducing interventions, and, critically, initiating the cascade testing conversation.
Cascade testing: from individual result to family-level risk management
When a pathogenic variant is identified, that result carries direct implications for first-degree relatives (parents, siblings, children), each of whom has a significant probability of carrying the same variant. Cascade testing — systematic testing of at-risk relatives — is the mechanism by which a single diagnosis is converted into family-wide risk reduction.
The counsellor’s role here extends beyond the patient in the room. Counsellors assist patients in communicating results to family members, often providing a letter or summary that the patient can share. In some settings, proactive outreach to relatives (with the index patient’s consent) is offered. The logistics of cascade testing in India present real challenges: geographic dispersion of families, varying access to testing across states, and social dynamics that can complicate disclosure. Acknowledging these barriers directly and offering practical communication support materially improves uptake.
At the population level, cascade testing is the mechanism that gives hereditary cancer programs their public health value. A BRCA2 mutation found in a 42-year-old woman with breast cancer is also relevant to her 38-year-old sister, her 19-year-old daughter, and her 45-year-old brother (for whom BRCA2 confers elevated risks for male breast, pancreatic, and prostate cancer), each of whom has a 50% risk of carrying the same mutation. Stopping at the index patient is a clinical and ethical missed opportunity.
True Negative Result
A true negative result — the patient has been tested for a known familial variant and does not carry it — is the most clinically interpretable outcome. Risk returns approximately to the population level. Relatives who have tested negative for a specific familial variant do not require mutation-carrier surveillance protocols.
The counselling task here is clarification: a true negative result does not mean zero risk of cancer. Sporadic cancers occur. Standard screening remains appropriate. The result simply means the patient is not at elevated hereditary risk for that specific variant.
Uninformative Negative Result
An uninformative negative, i.e., no pathogenic variant identified, no known familial variant to test against, is the most common and, frequently, the most difficult result to communicate. The patient may have a strong family history and has tested negative on a comprehensive panel. What does this mean?
Possibilities include: the family carries a mutation in an uncharacterized gene (the landscape of hereditary cancer gene discovery remains incomplete); a mutation exists in a region not captured by the panel; the family history reflects shared environmental or polygenic risk; or the family history is coincidental. None of these possibilities can be conclusively distinguished from a single negative result.
Management in this context is guided by clinical and family history, not by the test result. A patient with a first-degree relative with ovarian cancer and early-onset breast cancer affecting three family members does not move to average-risk surveillance on the basis of a negative BRCA test. The counselling session must convey this clearly — and document it.
Variant of Uncertain Significance (VUS)
A VUS result is a laboratory finding: a DNA change that is neither classified as pathogenic nor confirmed as benign. VUS rates on multi-gene panels typically range from 20–40%, depending on the gene and population. In South Asian populations, where variant databases are substantially less complete than in European populations, VUS rates are higher.
The VUS result is the most challenging communication task in genetic counselling. The instruction is consistent across guidelines: a VUS should not be used for clinical management decisions. Surveillance and risk-reducing interventions should be based on personal and family history and not on the VUS.
Patients who receive a VUS often interpret it as a positive result. They may make or request management decisions (including prophylactic surgery) on the basis of a variant that may ultimately reclassify as benign. The counsellor’s task is to hold the uncertainty without dismissing the patient’s anxiety — and to establish a mechanism for follow-up when reclassification occurs.
Reclassification tracking is a structural gap in many clinical programmes. Variants reclassify — in both directions — as population databases grow. Patients who received VUS results five years ago may have results that now carry a definitive classification. Systematic reclassification notification is an institutional responsibility, not an afterthought.

A Few Considerations for the Indian Clinical Context
Database representation: Variant classification relies on allele-frequency data from population databases. South Asian populations are underrepresented in gnomAD and ClinVar. This elevates VUS rates and makes novel variant interpretation more uncertain. Pathogenicity calls made on variant databases built predominantly from European populations carry an inherent limitation when applied to Indian patients.
Testing access and cascade logistics: Out-of-pocket costs remain a barrier to index testing and particularly to cascade testing. Genetic counsellors working in the Indian context need to be familiar with institutional subsidy programmes, government schemes, and the practical reality that relatives in smaller cities or rural areas may have no straightforward path to testing.
Disclosure dynamics: Family disclosure of hereditary cancer results engages dynamics that differ from Western clinical contexts: joint family structures, marriage considerations, and potential stigma. Genetic counsellors working with Indian families may need to facilitate conversations that involve more family members, more cultural negotiation, and more careful sequencing of disclosure than standard North American or European communication templates anticipate.
Insurance implications: Indian life insurance underwriting practices around genetic information are not consistently regulated. Patients should be counselled that results may be requested by insurers, and ideally, they should secure life insurance before genetic testing, where this is a concern.
After the Session: Documentation and Follow-Up
The post-counselling clinical note should capture: the indication for testing; the pedigree summary; the result and its classification; the management plan (including surveillance, risk-reduction options discussed, and referrals made); the cascade testing plan and which relatives have been identified; and a genetic counselling session that concludes with documentation of all the above elements and a plan to reach first-degree relatives constitutes a complete and comprehensive clinical encounter.
Your Post-Counselling Checklist
Every complete genetic counselling experience should conclude with a clear, documented clinical note for your medical records. Ensure your documentation explicitly includes:
- Your comprehensive, three-generation family tree (pedigree summary).
- Your official laboratory test result and its exact classification.
- A personalised management plan (including specific imaging schedules, lifestyle adjustments, or specialist referrals).
- A clear plan for cascade testing, identifying exactly which relatives should consider testing and providing the communication tools to reach them.
- A structured follow-up plan to monitor for future lab updates if you received a VUS result.
Medical disclaimer: This article is for general educational purposes only and does not constitute medical advice. Guidelines vary by centre, patient profile, and resource availability. Always consult a qualified oncologist or breast cancer specialist for individual guidance.
Karkinos Healthcare