Previous articles in this series walked you through the process of breast cancer diagnosis, i.e., what happens when a lump is found, what tests are done, and what results mean. Now we move to a question that sits behind all of that: why does breast cancer happen in the first place?
For some people, the answer is written in their genes. BRCA1 and BRCA2 are the most well-studied genetic causes of breast cancer. If you have recently received a BRCA test result, or a doctor has suggested you get tested, this article will explain what these genes do, what a mutation actually means for your health, and why the picture looks different for Indian patients than what most articles describe.
First: What Does BRCA Stand For?
BRCA stands for BReast CAncer gene. The name came from the disease it was first linked to when scientists discovered it in the early 1990s. BRCA1 was identified in 1994, and BRCA2 in 1995.
Despite the name, these are not typical cancer genes. They are actually protection genes, general DNA repair genes that happen to have been discovered through breast cancer research, and the name stuck. Men carry these genes too, which is why BRCA mutations raise prostate and pancreatic cancer risk in men as well.
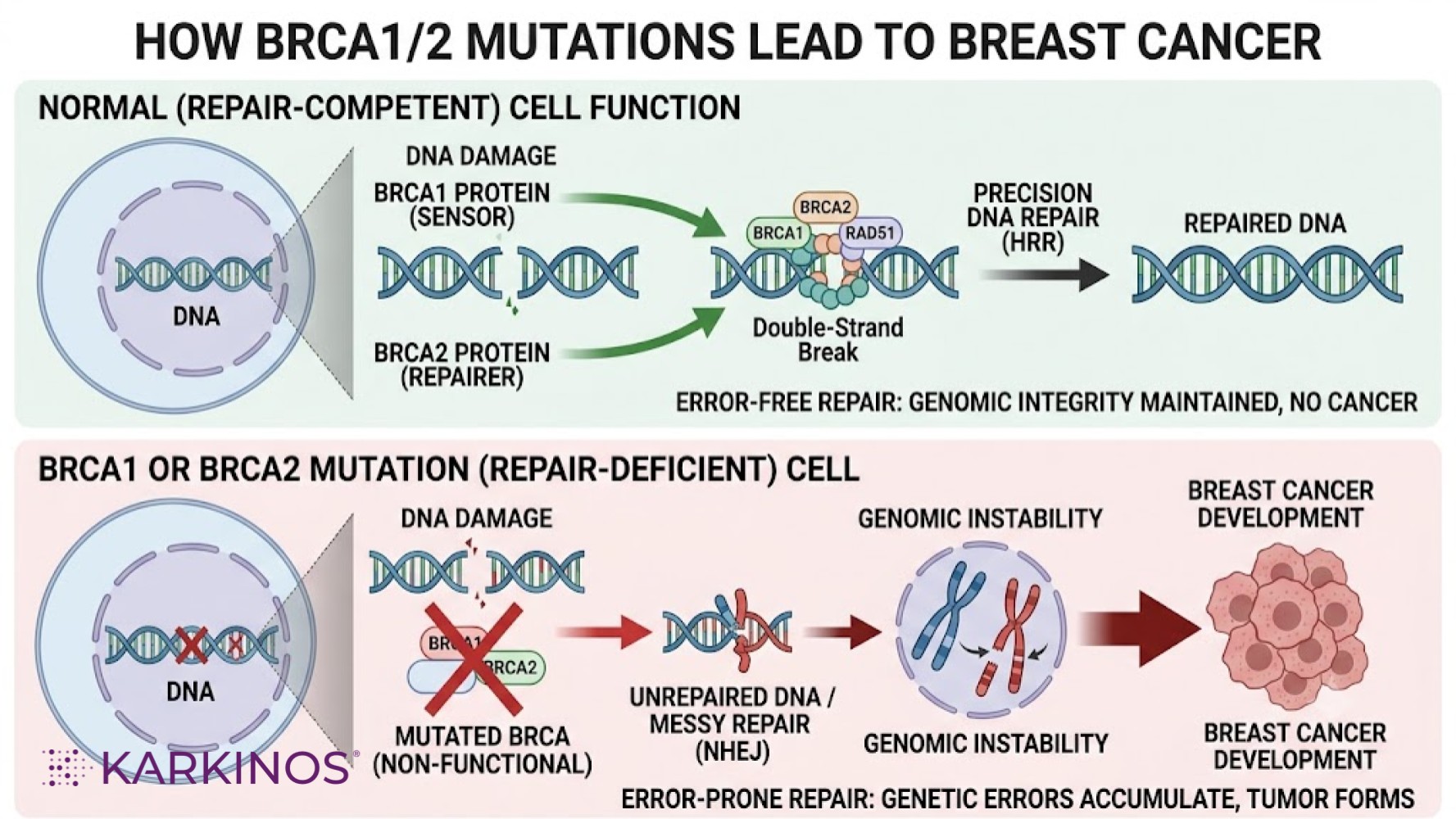 The repair process they lead is called Homologous Recombination Repair (HRR), in simple terms, a precise “copy-paste” repair system that fixes broken DNA using an exact backup copy as a template. It is the body’s most accurate method of DNA repair.
When your BRCA gene has a confirmed harmful change, one of these repair workers is missing or broken. The cell is then forced to fall back on emergency repair methods that are quick but messy, leaving behind mistakes. Over many years, those mistakes accumulate and can turn a normal cell into a cancer cell.
This is why BRCA mutations are linked to cancer, not because they directly cause it, but because they remove the body’s most important line of protection.
The repair process they lead is called Homologous Recombination Repair (HRR), in simple terms, a precise “copy-paste” repair system that fixes broken DNA using an exact backup copy as a template. It is the body’s most accurate method of DNA repair.
When your BRCA gene has a confirmed harmful change, one of these repair workers is missing or broken. The cell is then forced to fall back on emergency repair methods that are quick but messy, leaving behind mistakes. Over many years, those mistakes accumulate and can turn a normal cell into a cancer cell.
This is why BRCA mutations are linked to cancer, not because they directly cause it, but because they remove the body’s most important line of protection.
An important note: BRCA1 mutations are more likely to cause Triple-Negative Breast Cancer (TNBC), a type that is more aggressive and does not respond to hormone therapies. BRCA1 cancers also tend to appear at a younger age.
These numbers are not a verdict. They are a signal that closer monitoring and preventive care are important, and that early detection gives you the power to act at the right time.
Think of it like finding an unfamiliar word in a book. You cannot tell yet if it is a typo or just an unusual word — until you look it up. A VUS is science saying, “We need more information.”
Because of this, a VUS should not drive major medical decisions. Doctors manage a VUS the same way they manage a negative result, by using your personal and family history as the main guide.
VUS results are more common in Indian and South Asian patients because fewer South Asian genomes have been included in global reference databases. As more data is collected, many VUS results are eventually reclassified — most turn out to be harmless; a smaller number are found to be genuinely harmful.
This is why BRCA testing is not a one-time event. If you received a VUS result a few years ago, ask your doctor whether it has since been reclassified.
| A mutation is a permanent change in your body’s genetic instructions, essentially a typo (error) in the code that tells your cells how to grow and function. |
What Do BRCA1 and BRCA2 Actually Do?
Think of your body as a very large city. Every building is made up of millions of tiny bricks, i.e., your cells. Each cell contains a complete copy of your body’s instruction manual: your DNA. Every day, cells get small amounts of damage. Sun exposure, normal ageing, and even just breathing can cause tiny errors in DNA. Your body has dedicated repair workers whose job is to find this damage and fix it correctly before it causes any problems. BRCA1 and BRCA2 are two of the most important repair workers in your body. When DNA is damaged, BRCA1 is like the supervisor who arrives first at the scene. It sounds the alarm, stops the cell from dividing too quickly, and calls in the right team to start fixing things. BRCA2 is the specialist repair worker who then does the actual fixing. It ensures the DNA is repaired using an exact copy as a guide, so no mistakes are left behind.
The repair process they lead is called Homologous Recombination Repair (HRR), in simple terms, a precise “copy-paste” repair system that fixes broken DNA using an exact backup copy as a template. It is the body’s most accurate method of DNA repair.
When your BRCA gene has a confirmed harmful change, one of these repair workers is missing or broken. The cell is then forced to fall back on emergency repair methods that are quick but messy, leaving behind mistakes. Over many years, those mistakes accumulate and can turn a normal cell into a cancer cell.
This is why BRCA mutations are linked to cancer, not because they directly cause it, but because they remove the body’s most important line of protection.
What Does a BRCA Mutation Mean for Your Cancer Risk?
Carrying a BRCA mutation does not mean you have cancer, or that you will definitely get cancer. It means your protection system is weaker than average, and your lifetime risk is higher than that of the general population. Here is a simple way to understand the numbers: According to ICMR (Indian Council of Medical Research) data, about 1 in 28 Indian women will develop breast cancer in her lifetime — roughly 3 to 4 out of every 100. In urban areas, that number is slightly higher, at 1 in 22. For Indian women with a BRCA1 or BRCA2 mutation, that risk rises sharply, to roughly 50 to 72 out of 100 by age 70. That is nearly 15 to 20 times higher than the average Indian woman’s risk. BRCA1 and BRCA2 also carry different risk profiles from each other:| Cancer Type | General Population | BRCA1 Mutation | BRCA2 Mutation |
| Female Breast | ~3–4% (India) | 55–72% | 45–69% |
| Ovarian | ~1% | 39–60% | 11–30% |
| Male Breast | Very rare | ~1% | 5–10% |
| Prostate (men) | ~12% | Slightly elevated | Up to 25% |
| Pancreatic | ~1.5% | 1–3% | 2–7% |
How Do You Know If You Should Get Tested?
Most people who carry a BRCA mutation do not know it. There are no symptoms. The gene change is invisible until cancer appears or until you get tested. The starting point is not a symptom. It is your family history. Warning signs in your family history:- A mother, sister, or daughter diagnosed with breast cancer before age 50
- Any relative, at any age, with ovarian cancer
- Multiple relatives on the same side of the family with breast or ovarian cancer
- A male relative with breast cancer (rare in the general population; strongly linked to BRCA2)
- A relative with pancreatic cancer, especially alongside breast or ovarian cancer in the family
- A family member who has already tested positive for a BRCA mutation
- Breast cancer diagnosed at age 50 or younger
- Triple-negative breast cancer at any age
- Ovarian, pancreatic, or metastatic prostate cancer at any age
Why Indian Patients Are Different and Why This Matters
Most of what doctors know about BRCA mutations came from research on Ashkenazi Jewish communities in Eastern Europe. In that population, almost all harmful BRCA mutations are one of just three known types. Testing there is simple: check for three mutations, and you have a good answer. Indian patients are different. Research shows that in India, the types of BRCA mutations are far more varied. There is no small fixed list that covers most Indian cases. Indian patients carry many different mutations spread across both genes, and some are unique to Indian populations, not found in Western databases at all. Three things stand out specifically for Indian patients: Breast cancer appears younger. Indian women with BRCA mutations often develop cancer in their 40s, sometimes earlier. In Western studies, most cases appear after menopause, in the 60s. Indian women need to start monitoring earlier. BRCA1 is more common than BRCA2 in India, unlike the pattern seen in some Western populations. Triple-Negative Breast Cancer (TNBC) rates are higher. In India, 15–30% of TNBC cases are linked to BRCA mutations, a higher proportion than the global average. This makes BRCA testing particularly important for Indian women diagnosed with TNBC. Because Indian-specific data is still being collected, Indian patients need full gene sequencing (NGS), not the shorter panel test designed for Western populations. If a lab offers only a panel test, ask specifically whether it covers the full gene.What Is a Variant of Uncertain Significance (VUS)?
Sometimes a BRCA test comes back with a result called a Variant of Uncertain Significance, or VUS.| A VUS is not a positive result. It simply means: “We found a change in your DNA, but we do not yet know whether it is harmful or harmless.” |
Which is the right test?
The right test for Indian patients is the NGS (Next-Generation Sequencing) test, which reads the entire BRCA1 and BRCA2 genes, covering the full range of mutations rather than a limited panel.If You Test Positive: What Happens Next?
A positive BRCA result is serious but also actionable. Knowing about it gives you the chance to act before cancer develops. Options your doctor will discuss include: Earlier and more frequent screening. Women with BRCA mutations start breast cancer screening from age 25–30, with annual MRI scans in addition to standard mammograms. Research shows that MRI, when combined with mammography, detects 94% of cancers, compared with just 39% with mammography alone. Preventive medicines. Certain medicines can meaningfully lower breast cancer risk in high-risk women. Preventive surgery. Some women choose surgery to remove breast tissue or ovaries before cancer develops. For BRCA1 carriers, removing the ovaries before cancer appears reduces ovarian cancer risk by approximately 80%. This is a major decision requiring careful specialist guidance. For men with BRCA2. Regular prostate-specific antigen (PSA) testing from age 40 is recommended, as discussed with a doctor. For your family. Each child of a BRCA mutation carrier has a 50% chance of inheriting the mutation. Your siblings and adult children should be offered testing — this is called cascade testing.Whatever the result, genetic counselling is essential. A genetic counsellor will explain what your specific result means, what it means for your family, and help you build a realistic plan — without panic or confusion.