When we explored BRCA1 and BRCA2 in the previous blog, we looked at how genetic knowledge can completely change a family’s future. But science has moved forward, and testing for BRCA alone is no longer the gold standard.
Expanding our view beyond BRCA genes is not just about collecting more medical data. It is about giving women the exact roadmap they need to take action, start screenings early, and catch changes long before a tumour has a chance to grow.
Also, understanding genes beyond BRCA1 and BRCA2 is crucial for Indian women because the biological and genetic landscape of breast cancer in India looks very different from Western countries.
Here is why looking at the broader genetic picture is so important:
- Breast Cancer Hits Indian Women a Decade Earlier
- In Western nations, breast cancer is most common in women over the age of 60. In India, the disease strikes much earlier, with the average age at diagnosis ranging from 45 to 50 years.
- When breast cancer appears at a young age, it is far more likely to be driven by genetics.
If a young Indian woman tests negative for BRCA1 and BRCA2, she might assume she is in the clear. However, a high-risk mutation could still be lurking in another gene, like PALB2 or TP53.
- Non-BRCA Mutations Are Common in India
Recent clinical studies tracking Indian breast cancer patients show that focusing only on BRCA genes leaves a massive blind spot.
- Among Indian women who test positive for an inherited cancer gene, up to 34% of the mutations are found in non-BRCA genes (such as ATM, CHEK2, and PALB2).
- Testing only for BRCA1 and BRCA2 means that more than 1 in 3 hereditary cases could be completely missed.
- High Rates of Aggressive Subtypes
Indian women experience a higher rate of Triple-Negative Breast Cancer (TNBC), an aggressive subtype that grows quickly and requires definitive treatment.
- Certain non-BRCA genes are closely linked to these specific tumour types.
- Identifying these genes helps doctors choose precise, targeted treatments, such as PARP inhibitors for PALB2 mutations, rather than relying solely on standard chemotherapy.
- India’s Unique Genetic Diversity
Because of India’s vast population history and traditional community-based marriage patterns, the Indian genome has unique genetic traits.
- Many Indian families carry “founder mutations”—specific genetic changes unique to the subcontinent that do not show up in Western medical databases.
- Broad multi-gene testing helps identify these uniquely Indian variants, giving families a much more accurate picture of their actual risk.
- Overcoming Late Detection
The survival rate for breast cancer in India is lower primarily because tumours are often caught at an advanced stage.
- Knowing about non-BRCA gene mutations changes this timeline entirely.
- It gives high-risk families a roadmap to start intensive screenings (like breast MRIs) by age 30, shifting the focus from treating late-stage illness to prevention and early cure.
Hence, for families with a history of early-onset cancers, relying on standard BRCA testing alone is no longer enough. Moving to broad multi-gene panels provides the full picture needed to save lives through early action.
The other genes responsible for elevating breast cancer risk
A negative BRCA result does not mean zero hereditary risk. Five other genes, each with its own risk profile and clinical implications, can be just as consequential.
When a genetic test comes back BRCA-negative, the instinct is relief. But for many people with a strong family history of breast or ovarian cancer, that result leaves a question unanswered: why does this keep happening in my family? The answer could actually lie elsewhere in the genome.
Multi-gene panel testing, now widely available (including Karkinos Healthcare) and covered by several Indian insurance schemes under oncology benefits, can screen for dozens of genes simultaneously. Five of them are clinically significant enough to change surveillance plans, surgical decisions, and testing recommendations for relatives.
Why this matters now
Studies suggest that among BRCA-negative patients who have features of hereditary cancer (early onset, bilateral disease, multiple affected relatives), somewhere between 5% and 15% carry a pathogenic variant in one of these other genes.
The other major genes at a glance
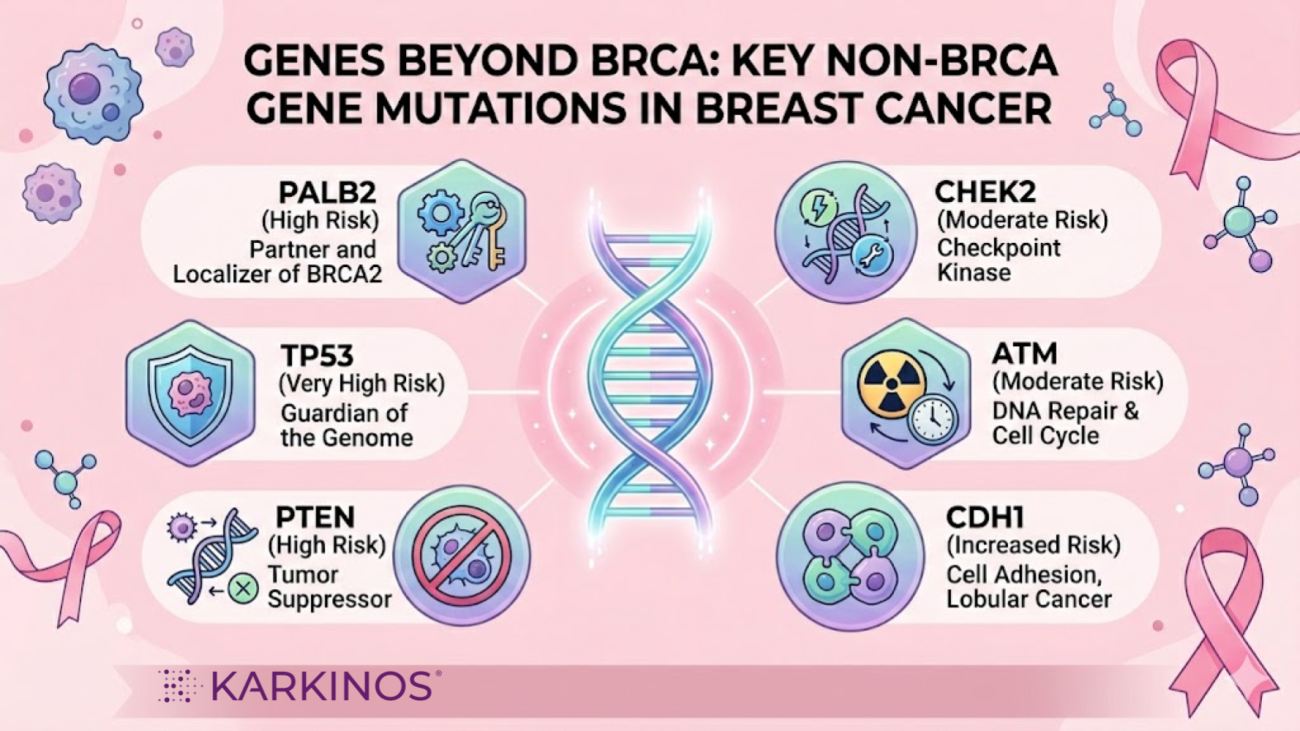
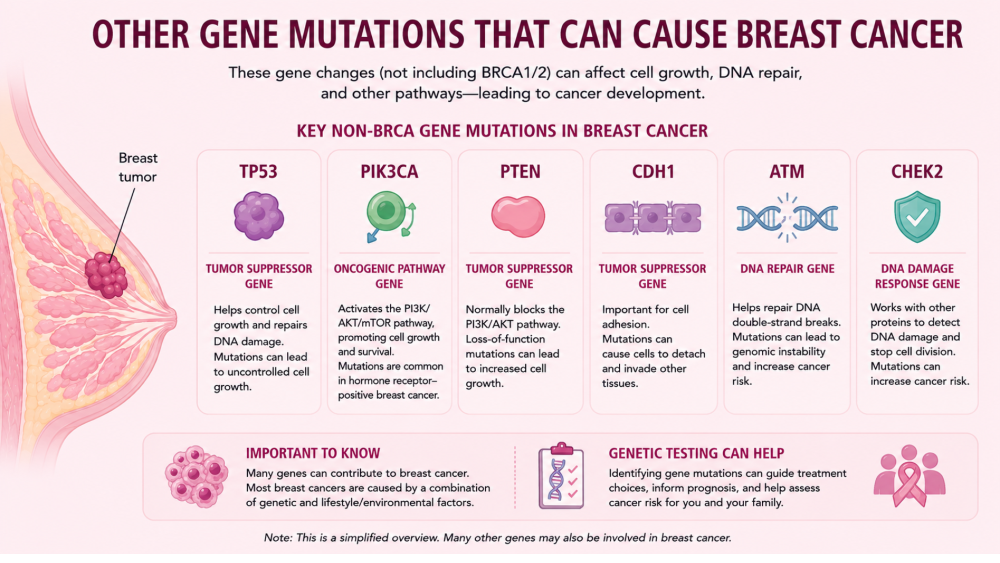
Beyond BRCA1 and BRCA2, there are several other genes that significantly increase a person’s risk of developing breast cancer when mutated.
We know that BRCA1 and BRCA2 are highly specialised repair workers with a very specific job: fixing broken DNA strands. Just like those two famous genes, every other gene in the list below also has a specific, critical job to do to keep a cell healthy. Some act as first responders to detect DNA damage, some act as brakes to stop cells from growing too fast, and others act as a clean-up crew that tells severely damaged cells to self-destruct.
When these non-BRCA genes mutate and stop performing their assigned functions, errors accumulate in the DNA. This causes the uncontrolled cell growth that eventually turns into cancer.
Based on the level of risk they pose, these genes generally fall into two main categories: high-risk and moderate-risk.
TABLE: GENES INVOLVED IN BREAST CANCER
| Category | Gene | Normal Cellular Function | Lifetime Breast Cancer Risk for Carriers | Other Associated Cancers / Conditions |
| High Risk (High Penetrance) | PALB2 | Connects BRCA1 and BRCA2 to repair broken DNA strands. | 35% to 60% | Pancreatic cancer, male breast cancer, Fanconi anemia (if both copies mutated). |
| TP53 | “Guardian of the genome”; stops cell division or triggers cell suicide when DNA is damaged. | 56% to 90% (Often very early onset) | Li-Fraumeni Syndrome; sarcomas, brain tumors, leukemia, bone cancer. | |
| PTEN | Acts as a cellular brake to control how quickly cells grow and divide. | 25% to 85% | Cowden Syndrome; thyroid, endometrial (uterine), kidney, and colorectal cancers. | |
| CDH1 | Helps cells stick together and suppresses tumours by maintaining tissue organisation. | 40% to 50% (Specifically Invasive Lobular Carcinoma) | Hereditary Diffuse Gastric (stomach) Cancer. | |
| STK11 | Regulates cell shape, organisation, and chemical energy levels. | 45% to 54% | Peutz-Jeghers Syndrome; colorectal, pancreatic, stomach, and small intestine cancers. | |
| Moderate Risk (Moderate Penetrance) | CHEK2 | Acts as a DNA damage sensor; it pauses the cell cycle to allow for repairs. | Doubles the risk (~20% to 30% lifetime risk) | Estrogen Receptor-positive (ER+) breast cancer, male breast cancer, and colorectal cancer. |
| ATM | “First responder” that detects major DNA breaks and coordinates the repair response. | 20% to 40% | Pancreatic cancer; Ataxia-Telangiectasia (if both copies mutated). | |
| BARD1 | Binds directly to BRCA1 to stabilise it and help it suppress tumours. | Doubles the risk | Associated with Triple-Negative Breast Cancer (TNBC). | |
| RAD51C | Works with BRCA proteins to physically repair damaged DNA strands. | Modestly elevated risk | Highly associated with ovarian cancer and Triple-Negative Breast Cancer (TNBC). | |
| RAD51D | Works alongside RAD51C to repair double-strand DNA breaks. | Modestly elevated risk | Highly associated with ovarian cancer and Triple-Negative Breast Cancer (TNBC). |
Category 1: High-Penetrance (High-Risk) Genes
Mutations in these genes carry a substantial lifetime risk of breast cancer, often comparable to or approaching the risk associated with BRCA mutations.
- PALB2 (Partner and Localizer of BRCA2)
- The Function: PALB2 acts as the crucial bridge between BRCA1 and BRCA2. It localises the BRCA2 protein to the site of DNA damage, allowing the DNA to be repaired properly. Without PALB2, the entire BRCA DNA repair pathway fails.
- The Breast Cancer Risk: Often called “the third BRCA gene.” For women who carry a mutated PALB2 gene, the lifetime risk of developing breast cancer is estimated to be between 35% and 60%. The risk increases significantly if there is a strong family history of breast cancer.
- Other Associated Cancers: Pancreatic cancer and male breast cancer. (Inheriting two mutated PALB2 genes — one from each parent — causes a severe condition called Fanconi Anaemia subtype N).
- TP53 (Tumour Protein p53)
- The Function: Known as the “Guardian of the Genome.” This gene detects DNA damage and halts cell division to allow for repair. If the damage is too extensive, TP53 triggers cell suicide (apoptosis) to prevent the cell from becoming cancerous.
- The Breast Cancer Risk: Mutations cause Li-Fraumeni Syndrome (LFS). Women with LFS have a highly elevated lifetime risk of breast cancer, often approaching 85-90%. A distinguishing feature is an incredibly early onset, frequently before age 30, and the Triple-Negative subtype is often present.
- Other Associated Cancers: Bone cancer (osteosarcoma), soft tissue sarcoma, brain tumours, and leukaemia. Standard radiation therapy is often discouraged as it can trigger new tumours in these patients.
- PTEN (Phosphatase and Tensin Homolog)
- The Function: PTEN acts as a vital brake on cell growth and division. It regulates a signalling pathway that tells cells when to grow and when to stop.
- The Breast Cancer Risk: Mutations cause Cowden Syndrome (part of PTEN Hamartoma Tumour Syndrome). The lifetime risk of breast cancer for women is estimated at 25% to 85%.
- Other Associated Cancers: High risks for thyroid cancer and endometrial (uterine) cancer, as well as kidney and colorectal cancers. Benign growths (hamartomas) on the skin and inside the mouth are common clinical signs.
- CDH1 (Cadherin 1)
- The Function: This gene creates a protein (E-cadherin) that helps cells stick together to form organised tissues. It is essential for maintaining tumour suppression by keeping cells in their proper place.
- The Breast Cancer Risk: Mutations cause Hereditary Diffuse Gastric Cancer (HDGC) syndrome. The risk here is specifically for Invasive Lobular Carcinoma (ILC), which starts in the milk-producing lobules. The lifetime risk of ILC for women is estimated at 40% to 50%.
- Other Associated Cancers: Highly associated with diffuse (scattered) gastric (stomach) cancer, often at a young age.
- STK11 (Serine/Threonine Kinase 11)
- The Function: STK11 helps regulate cell polarity (the shape and organisation of cells) and energy metabolism. It also acts as a tumour suppressor.
- The Breast Cancer Risk: Mutations cause Peutz-Jeghers Syndrome (PJS). The lifetime risk of breast cancer is significantly elevated, estimated at 45% to 54%.
- Other Associated Cancers: High risk for colorectal, pancreatic, stomach, and small intestine cancers, as well as unique ovarian and testicular tumours. A classic sign is dark freckling on the lips and inside the mouth.
Category 2: Moderate-Penetrance (Moderate-Risk) Genes
Mutations in these genes roughly double or triple the risk of breast cancer compared to the general population. They are also involved in DNA repair pathways.
- CHEK2 (Checkpoint Kinase 2)
- The Function: This gene acts as a DNA damage sensor. When DNA is damaged, CHEK2 activates TP53 (the Guardian) and other repair genes to pause the cell cycle.
- The Breast Cancer Risk: Roughly doubles the lifetime risk for women, up to about 20-30%. The risk is especially linked to Estrogen Receptor-positive (ER+) tumours.
- Other Associated Cancers: Significantly increases male breast cancer risk (roughly 10-fold) and is associated with colorectal cancer.
- ATM (Ataxia-Telangiectasia Mutated)
- The Function: ATM is the “first responder” that detects major DNA damage (double-strand breaks) and signals other genes (such as CHEK2 and BRCA1) to initiate DNA repair.
- The Breast Cancer Risk: Mutations double or triple the lifetime risk, up to about 20-30%.
- Other Associated Cancers: Pancreatic cancer. Inheriting two mutated ATM genes causes Ataxia-Telangiectasia, a severe neurological disorder.
- BARD1 (BRCA1-Associated RING Domain 1)
- The Function: BARD1 binds directly to BRCA1. They form a complex that is essential for BRCA1’s stability and tumour-suppressive activity. If BARD1 is missing, BRCA1 cannot function.
- The Breast Cancer Risk: Recent data indicate this is a moderate-risk gene, roughly doubling the lifetime risk. It is often associated with Triple-Negative Breast Cancer (TNBC).
- RAD51C & RAD51D
- The Function: Both genes are part of the RAD51 family, which works alongside the BRCA proteins to physically repair broken DNA strands through homologous recombination.
- The Breast Cancer Risk: These genes have long been established as high-risk for ovarian cancer, but newer data confirm they are also moderate-risk genes for breast cancer, specifically the Triple-Negative subtype.
Why a multi-gene panel test is essential
Testing only for BRCA1 and BRCA2 misses all the risks listed above. When a patient uses a comprehensive multi-gene panel, they can learn if they have a mutation in any of these genes. This knowledge changes everything:
- Earlier Screening: Patients begin screening at ages 25-30 (often using Breast MRI).
- Specific Surveillance: If the gene is CDH1, surveillance focuses on Lobular cancers; if it’s STK11, screening includes the colon and pancreas.
- Targeted Treatment: Mutations in PALB2 and ATM may respond well to specialised drugs such as PARP inhibitors, similar to BRCA mutations.
When should you request a multi-gene panel test?
Guidelines from NCCN and the European Society of Medical Oncology (adapted for Indian practice by some oncology centres) typically suggest multi-gene panel testing when:
- A BRCA test was negative, but cancer in personal or family history remains strongly suggestive.
- Multiple first- or second-degree relatives with breast, ovarian, pancreatic, or prostate cancers; bilateral breast cancer; triple-negative breast cancer under 60; male breast cancer. Any of these in a BRCA-negative context warrants broader testing.
- Breast cancer before age 40. Early onset is one of the strongest indicators of hereditary risk, regardless of family history. Many young patients have de novo (from the beginning) pathogenic variants with no prior family signal.
- Unusual cancer combinations in the family. Breast plus thyroid plus endometrial points toward PTEN; breast plus sarcoma or brain tumour in a young relative points toward TP53; breast plus pancreatic points toward PALB2, ATM, or BRCA2.
- A known variant in the family (even in a distant relative). If any relative has tested positive for a pathogenic variant, all first-degree relatives should be offered targeted testing for that specific variant, ideally before cancer develops.
If your family has a history of early-onset cancers, a negative BRCA test is only half the story. Speak to an oncologist or a genetic counsellor today about comprehensive multi-gene panel testing to uncover your complete genetic roadmap. Taking action now can pave the way for earlier screening, targeted care, and true peace of mind for you and your loved ones.
References
Beyond BRCA: What a Major Indian Study Reveals About Hidden Genetic Risks in Breast Cancer