
HER2 is a molecule that significantly influences the behaviour of certain types of breast cancer. Understanding HER2 helps explain why some tumours grow rapidly and exhibit aggressive characteristics.
What exactly is HER2?
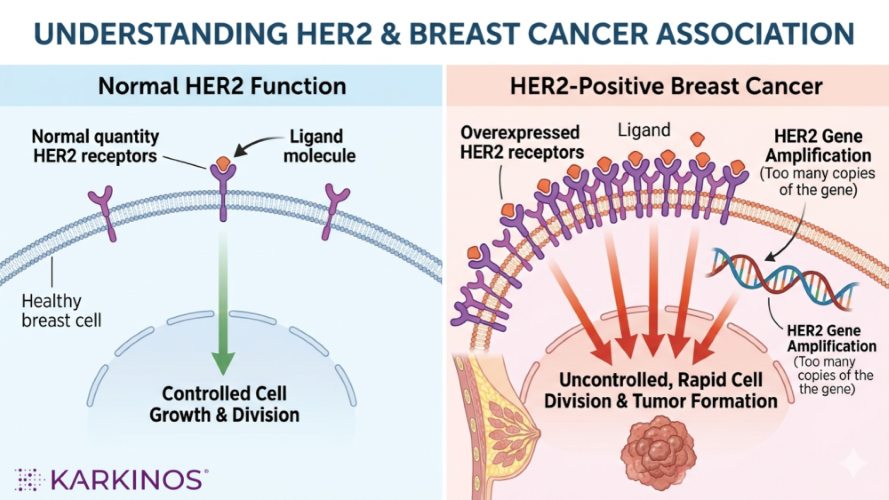
HER2 (Human Epidermal Growth Factor Receptor 2) is a protein found on the surface of breast cells. It belongs to a family of receptors that regulate how cells grow, divide, and repair themselves. In healthy cells, HER2 signalling is tightly controlled, functioning as a growth-regulatory switch.
To explain in detail, every cell in our body contains a copy of the HER2 gene (formally known as ERBB2), which encodes a protein located in the cell membrane. This protein is like an antenna. When growth signals from the surrounding environment bind to it, HER2 sends a “divide now” command into the cell’s interior.
Normally, a healthy cell has about 20,000 to 50,000 of these receptors on its surface. This amount is sufficient to respond to valid growth signals without causing the cell to become dysfunctional.
Amplification vs. expression — a critical distinction
This is the most important conceptual distinction in HER2 biology. Gene expression means the gene is being read and turned into a protein. Every normal cell expresses HER2 at a low level. Even some cancers can show mildly elevated HER2 protein without true amplification.
Gene amplification is different and far more ominous. It means the physical DNA segment containing the HER2 gene has been duplicated — sometimes dozens of times — within the cancer cell’s chromosomes.
Instead of the usual 2 copies of the gene (one from each parent), an amplified cancer cell may carry 20, 40, or even over 100 copies. Each of those copies gets transcribed and translated, so the cell ends up manufacturing an astronomical number of HER2 receptor proteins, sometimes over a million per cell, compared to tens of thousands in a normal cell.
The amplification typically occurs on chromosome 17q12, where the HER2 gene lives. The chromosome region is physically rearranged, sometimes as extra-chromosomal “mini-chromosomes,” sometimes as tandem repeats within the chromosome itself (called homogeneous staining regions, or HSRs). This kind of growth is known to be a genomic catastrophe, not just a regulatory glitch.
What goes wrong in HER2-positive cancer?In about 15–20% of breast cancers, the HER2 gene is amplified (extra copies), which leads to:
Think of it as a growth accelerator stuck to the floor. |
Why amplification drives aggressive disease
With a million antennas instead of 40,000, the receptor no longer needs an external signal. At that density, HER2 receptors begin spontaneously pairing with each other (homodimerization) or with other HER family members (heterodimerization with HER1/EGFR, HER3, HER4). These pairings fire off growth signals constantly, even in the complete absence of the normal ligands that are supposed to activate them. The cell receives an unrelenting “divide” command.
Normally, the body carefully controls when cells grow and when damaged cells should die. But when these control systems fail, it is like a car with the accelerator stuck down and the brakes disconnected. Cells begin growing and dividing far too quickly, while the usual signals that tell unhealthy cells to stop or die are ignored. As this uncontrolled growth continues, the rapidly multiplying cells make more mistakes in their DNA, allowing the cancer to become more aggressive over time.
This explains why HER2-amplified cancers tend to have a higher nuclear grade, higher proliferative index (Ki-67), and greater metastatic potential than HER2-negative cancers of the same histologic type. It also explains why HER2-targeting drugs like trastuzumab work: they bind the extracellular domain of the protein, partially blocking receptor dimerisation and flagging the cancer cell for immune destruction.
One of the most remarkable facts about HER2-positive breast cancer is that it went from being considered one of the most aggressive forms of breast cancer to one of the biggest success stories in targeted cancer therapy.
Before HER2-targeted drugs were developed, HER2-positive cancers were associated with high recurrence rates and poorer survival. The introduction of trastuzumab (Herceptin) dramatically changed outcomes by specifically targeting the HER2 protein, transforming treatment and significantly improving survival for many patients worldwide.
HER2 Diagnostics
HER2 diagnostics play a critical role in modern breast cancer care because the test result directly influences treatment decisions. HER2-positive cancers tend to grow faster and behave more aggressively, but they may also respond exceptionally well to targeted therapies specifically designed to block the HER2 pathway. Accurate testing, therefore, becomes essential in ensuring that patients receive the most appropriate treatment.
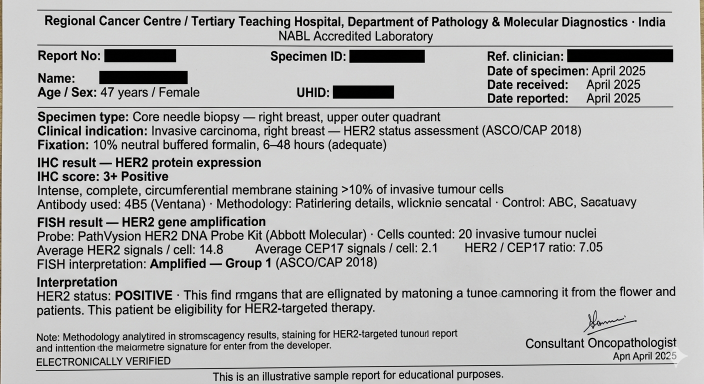
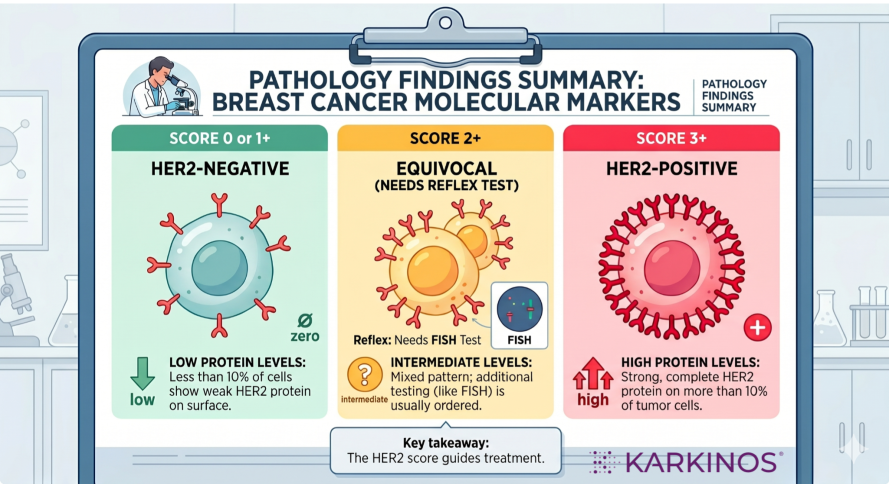
HER2 testing is usually performed on tumour tissue using two main methods. Immunohistochemistry (IHC) measures the amount of HER2 protein present on the surface of cancer cells and is reported as scores ranging from 0 to 3+.
When results are borderline or equivocal, another test, In Situ Hybridisation (ISH/FISH), is used to determine whether the HER2 gene itself is amplified within the tumour cells.
The precision of HER2 diagnostics is extremely important. A false-negative result may prevent a patient from receiving potentially life-saving targeted therapy, while a false-positive result may expose patients to unnecessary treatment and expense. For this reason, proper tissue handling, fixation, laboratory quality standards, and expert interpretation are all essential parts of accurate HER2 assessment.
HER2 diagnostics also represent one of the earliest and most successful examples of precision oncology, where a molecular test directly guides targeted treatment. More recently, the emergence of “HER2-low” breast cancer has further expanded the importance of HER2 testing, as newer therapies are showing benefit even in tumours previously considered HER2-negative.
Table 1
HER2 IHC Scoring and Clinical Interpretation
| IHC Score | What the Pathologist Sees | What It Means | HER2 Status | Next Step |
| 0 | No staining, or extremely faint staining in less than 10% of tumour cells | HER2 protein is essentially absent or present only at normal background levels | HER2 Negative | No further HER2 testing is usually needed |
| 1+ | Faint, incomplete staining in more than 10% of tumour cells | Small amounts of HER2 protein are present, but not enough to indicate true overexpression | HER2 Negative (though now clinically relevant as “HER2-low” in some newer therapies) | No traditional HER2-targeted therapy eligibility |
| 2+ | Moderate or incomplete staining that is not clearly negative or clearly positive | The “equivocal” or borderline category — protein levels alone cannot determine whether true HER2 gene amplification exists | Indeterminate | Requires confirmatory molecular testing with FISH/ISH |
| 3+ | Strong, dark, complete membrane staining in more than 10% of tumour cells | HER2 protein is massively overexpressed | HER2 Positive | Eligible for HER2-targeted therapy |
HER2 and the Evolution of Precision Diagnostics
HER2 transformed the understanding of breast cancer by demonstrating that cancers are not all biologically alike. Tumours driven by HER2 amplification tend to grow faster, divide more aggressively, and spread more readily because the cellular “growth signals” remain continuously switched on.
Yet this same biological vulnerability also became one of oncology’s greatest therapeutic successes, as targeted anti-HER2 therapies dramatically changed outcomes for patients worldwide.
Equally important was the evolution of HER2 diagnostics, which became inseparable from treatment itself. Techniques such as IHC and FISH moved breast cancer care beyond diagnosis based purely on microscopic appearance and into the era of molecular precision medicine.
Today, accurate HER2 testing does far more than classify a tumour; it determines therapeutic eligibility, guides clinical decisions, and helps match patients to treatments specifically designed for their disease biology.
Together, HER2 biology and HER2 diagnostics illustrate a defining shift in modern cancer care: understanding the molecular drivers of a tumour can fundamentally alter both prognosis and treatment strategy.
Medical disclaimer: This article is for general educational purposes only and does not constitute medical advice. Guidelines vary by centre, patient profile, and resource availability. Always consult a qualified oncologist or breast cancer specialist for individual guidance.
Karkinos Healthcare