Have you ever thought about what defines a woman, how her body is shaped, and how her tissues are prepared for her life’s most important roles? The answer begins not with what we see on the surface, but with what happens at the cellular level, driven by two powerful hormones: oestrogen and progesterone.
Hormones are the body’s chemical messengers, travelling through the bloodstream to deliver instructions that regulate how cells grow, function, and respond to change. In women, oestrogen and progesterone are among the most influential of these messengers.
Secreted primarily by the ovaries, both hormones work in a carefully coordinated balance, governing reproductive development, shaping body composition, and influencing tissues far beyond the reproductive system. When this balance is intact, the body functions as it should. When this balance is disrupted, the effects can be seen in many parts of the body, especially in the breasts.
Understanding the structural details of the hormones
Before exploring how these hormones influence the breast, it is essential to understand the cellular landscape they act upon. The functional units of the breast, the ducts and lobules, are lined by an inner layer of luminal epithelial cells that surround a central hollow space called the lumen and an outer layer of myoepithelial cells that provide structural support.
Among these, luminal cells are the most biologically significant in the context of hormone action. They are selectively equipped with oestrogen receptors (ER) and progesterone receptors (PR), making them highly responsive to circulating hormonal signals.
These receptors act as molecular switches. When oestrogen binds to ER, it activates gene programmes that drive cell proliferation and ductal growth. When progesterone binds to PR, it promotes differentiation, maturation, and structural organisation. The presence and activity of these receptors determine how breast tissue responds across the menstrual cycle, pregnancy, and menopause.
Importantly, most breast cancers arise from hormone-responsive luminal cells that retain these receptors, which continue to influence tumour behaviour.
These hormones are central to breast biology and breast cancer risk, but they do not fit into a simple good or bad category. Instead, they function as powerful regulators of breast tissue behaviour, capable of both maintaining health and contributing to disease depending on their balance, timing, and cumulative exposure.
Breast cancer subtypes by receptor status
| Subtype | ER | PR | HER2 | Prevalence | Key features & treatment |
| Luminal A
Most common subtype |
Positive | Positive | Negative | ~40–50% of cases | Low proliferation rate. Best prognosis. Responds well to hormone therapy (tamoxifen, aromatase inhibitors). Chemotherapy is often not needed. |
| Luminal B (HER2−) | Positive | Low / variable | Negative | ~15–20% of cases | Higher proliferation than Luminal A. Intermediate prognosis. Hormone therapy ± chemotherapy. |
| Luminal B (HER2+) | Positive | Variable | Positive | ~10% of cases | More aggressive. Hormone therapy + anti-HER2 therapy (trastuzumab) + chemotherapy. |
| HER2-enriched | Negative | Negative | Positive | ~15–20% of cases | Fast growing. No hormone receptor target. Anti-HER2 therapy + chemotherapy. Prognosis improved significantly with targeted therapy. |
| Triple Negative (TNBC)
Basal-like |
Negative | Negative | Negative | ~10–15% of cases | Most aggressive. No hormonal or HER2 target. Relies on chemotherapy. Immunotherapy emerging. Linked to BRCA1 mutations. |
What the receptors mean
| Receptor | What it is | Role in cancer | Targeted by |
| ER (ERα) | Estrogen receptor alpha — found on luminal breast cells | Estrogen binds ER and drives tumour cell proliferation in ER+ cancers | Tamoxifen (SERM), aromatase inhibitors (letrozole, anastrozole), fulvestrant (SERD) |
| PR | Progesterone receptor — expressed only when ER is present and active | Its presence confirms active ER signalling. High PR = better prognosis in ER+ cancers | Indirectly via anti-estrogen therapy; PR expression falls when ER is blocked |
| HER2 | Human epidermal growth factor receptor 2 — a growth-promoting protein on the cell surface | Overexpression drives aggressive, fast-dividing tumours. Unrelated to estrogen/progesterone pathways | Trastuzumab (Herceptin), pertuzumab, lapatinib, T-DM1 |
Beyond oestrogen and progesterone, a third hormone receptor, the Androgen Receptor (AR), plays a significant yet often overlooked role in breast health.
While androgens like testosterone are typically associated with men, they are also present in women and are found in the majority of both healthy and cancerous breast tissues.
In a balanced state, these receptors can act as a natural check against the growth-stimulating effects of oestrogen. However, in the context of breast cancer, the role of AR is more complex; it can sometimes slow down tumour growth in certain subtypes, while in others, particularly in some triple-negative cases, it may act as an alternative driver for the disease.
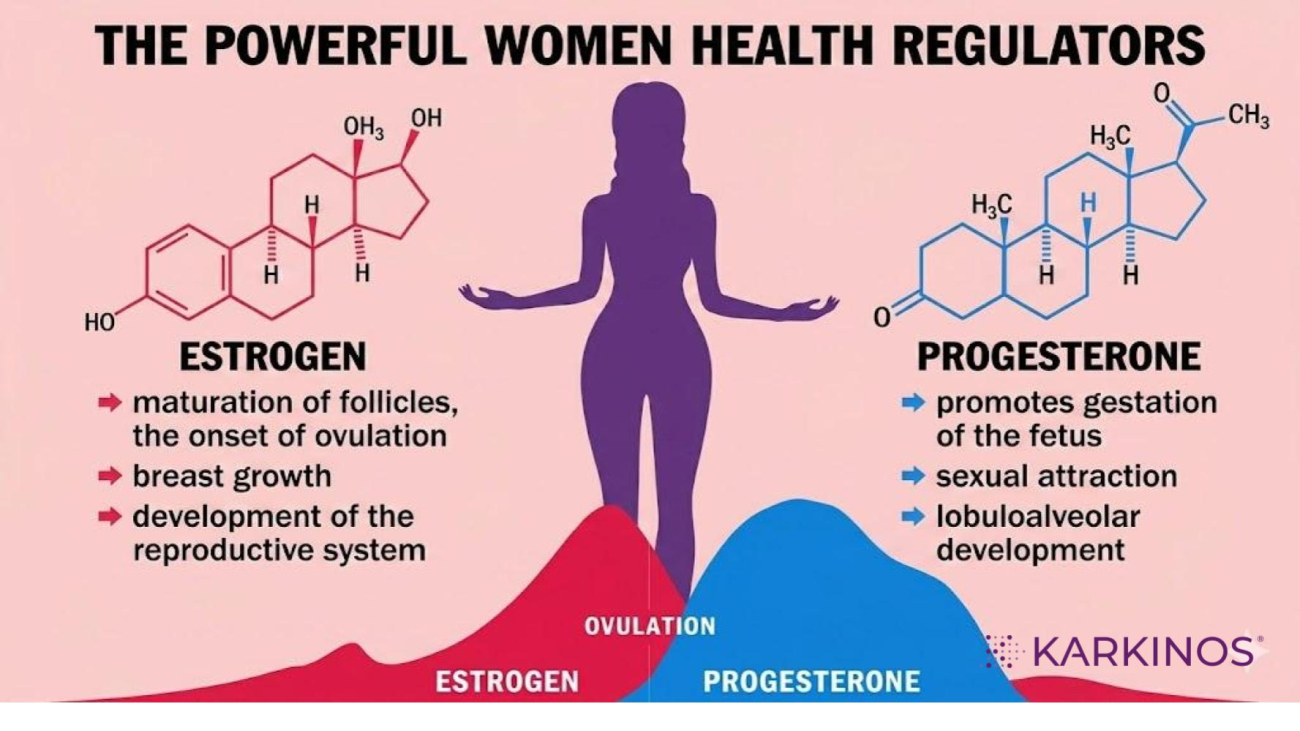
Functions of Oestrogen
Oestrogen is the primary hormone for breast growth and development. From puberty onward, it stimulates ductal expansion, increases cell proliferation in the breast epithelium, and enhances blood flow and connective tissue formation.
It also plays vital roles beyond the breast, including maintaining bone density, regulating lipid metabolism, influencing insulin sensitivity, and supporting cardiovascular health. However, its growth-promoting effect is inherently a double-edged phenomenon (something that has both positive and negative consequences).
Over a lifetime, prolonged or unopposed oestrogen exposure, seen in situations such as early menarche, late menopause, obesity, or certain forms of hormone therapy, can increase the likelihood of DNA replication errors. In simple terms, oestrogen drives cell division, and more division creates more opportunities for mutations to bring a change in the DNA sequence. This is why many breast cancers are classified as hormone receptor positive (HR+ve), meaning they grow in response to oestrogen signalling.
Functions of Progesterone
Progesterone, often less emphasised, plays an equally important but more regulatory role. Its primary function in the breast is to promote lobuloalveolar development, preparing the glandular tissue for potential milk production.
Beyond structural changes, progesterone drives cellular differentiation, guiding breast cells toward more mature and specialised states. This is significant because well-differentiated cells are generally less prone to malignant transformation than rapidly dividing, less specialised cells.
Progesterone also modulates oestrogen’s effects by controlling excessive proliferation and supporting controlled growth cycles. Systemically, it regulates the menstrual cycle, supports pregnancy, influences mood through neurosteroid pathways, and contributes to immune regulation.
Simply put, oestrogen builds while progesterone refines. Oestrogen expands the ductal framework of the breast, while progesterone shapes and organises it by developing lobules and alveoli. This relationship is not independent but deeply interconnected. Oestrogen induces the expression of progesterone receptors, which means progesterone’s actions depend on prior Oestrogen signalling.
Influence of hormones on the breast
During a woman’s reproductive years, breast tissue constantly changes due to hormone levels. Each month, the menstrual cycle features a growth phase, followed by a phase where cells mature and turnover is controlled. This dynamic process ensures that tissue growth remains regulated rather than excessive. The breast, in many ways, becomes a living record of a woman’s hormonal history.
This balance becomes even more pronounced during pregnancy. Oestrogen dramatically expands the ductal network, while progesterone drives the proliferation of lobular alveolar units in preparation for lactation. Interestingly, it is not the presence of these hormones but a shift in their levels that initiates milk production. After childbirth, the sharp drop in progesterone removes its inhibitory effect, allowing prolactin to trigger lactation.
The interplay between oestrogen and progesterone is where the real story of breast cancer risk lies. In a healthy physiological state, such as regular ovulatory cycles, oestrogen stimulates growth, and progesterone follows to stabilise, organise, and differentiate that growth.
When the balance of hormones in the body is disrupted, it can lead to changes in the biological environment. Chronic anovulation, which means not releasing eggs, results in low progesterone levels. This causes increased or sustained estrogen exposure, leading to ongoing cell growth signals.
Additionally, obesity after menopause can raise estrogen levels because fat tissue can convert other hormones into estrogen, further disrupting the balance. Over time, these conditions create a hormonal environment that increases the risk of abnormal cell growth, especially when combined with genetic and metabolic risk factors.
Oestrogen and progesterone do not act in isolation from lifestyle and environment. Chronic stress can elevate cortisol levels, which can interfere with progesterone production. Excess body fat increases oestrogen levels. Impaired liver function can reduce the body’s ability to clear hormones efficiently, allowing oestrogen to accumulate.
Environmental exposures, such as endocrine-disrupting chemicals found in plastics, pesticides, and personal care products, can mimic oestrogen and add to the hormonal burden. Nutrition, sleep, and metabolic health further influence how these hormonal signals are regulated.
Why is an imbalance in hormone secretion a problem?
For many women, the earliest signs of imbalance appear in the menstrual cycle. Irregular, painful, or unpredictable periods from menarche (onset of periods) often reflect underlying disruptions in how oestrogen is produced, regulated, or received by target tissues.
Too little oestrogen may lead to scanty or delayed cycles, while excess oestrogen can result in heavy or prolonged bleeding. These changes are not isolated uterine issues but signals of a broader hormonal imbalance affecting the entire reproductive axis.
The implications of this imbalance extend to breast health. Because breast tissue is highly sensitive to hormonal signals, prolonged exposure to elevated oestrogen without adequate progesterone-mediated regulation can drive excessive cell proliferation.
Over time, this increases the likelihood of abnormal growth patterns. Hormone receptor-positive breast cancers, the most common subtype, arise within this context, where the same hormonal pathways that support normal development can, when dysregulated, contribute to disease progression.
Understanding these mechanisms is central not only to breast cancer risk but also to prevention and treatment. Managing lifetime hormonal exposure through maintaining a healthy weight, supporting metabolic health, limiting unnecessary hormone therapy, and addressing lifestyle factors remains one of the most meaningful ways to influence risk.
At the same time, modern therapies such as anti-oestrogen agents and aromatase inhibitors are built on this understanding, targeting the hormonal pathways that tumours depend on.
Hence, oestrogen and progesterone are not simply protective or harmful. They are master regulators of breast tissue dynamics. Oestrogen drives growth. Progesterone refines and stabilises it. When balanced, they sustain normal physiology.
When disrupted, they can reshape the biological environment in ways that increase vulnerability to disease. Their importance lies not in isolation but in their interaction, which defines the terrain in which breast health is either maintained or compromised.
Medical disclaimer: This article is for general educational purposes only and does not constitute medical advice. Guidelines vary by centre, patient profile, and resource availability. Always consult a qualified oncologist or breast cancer specialist for individual guidance.
Karkinos Healthcare