
Understanding breast anatomy is essential for good breast health. Every woman and adolescent girl should be informed about the structure of the breasts to maintain good breast health throughout their lives.
Before a woman can identify what is abnormal, she needs to have a clear understanding of what is considered normal, i.e., how the breast is structured, how it functions, and how it changes throughout every phase of her life. For Indian women in particular, this understanding is not only medically important but often overlooked.
Much of the existing literature is based on Western data; however, Indian women possess unique body compositions, hormonal patterns, and epidemiological (public health-related) profiles that every woman must know to make informed decisions.
This blog, therefore, offers a foundational overview of breast anatomy and physiology, with a focus on features relevant to the average Indian woman.
Structure of the Breast
The breast is a glandular organ located on the anterior chest wall, overlying the pectoralis major muscle (a large, fan-shaped muscle located in the upper chest. This muscle is responsible for the movement of the shoulder joint and plays a key role in activities such as pushing, lifting, and rotating the arm.)
Each breast extends roughly from the second to the sixth rib vertically, and from the lateral border of the sternum (breastbone) to the mid-axillary line horizontally.
A small extension called the axillary tail reaches towards the armpit — a detail of clinical importance, as breast tissue at this location can sometimes be mistaken for a lymph node swelling.
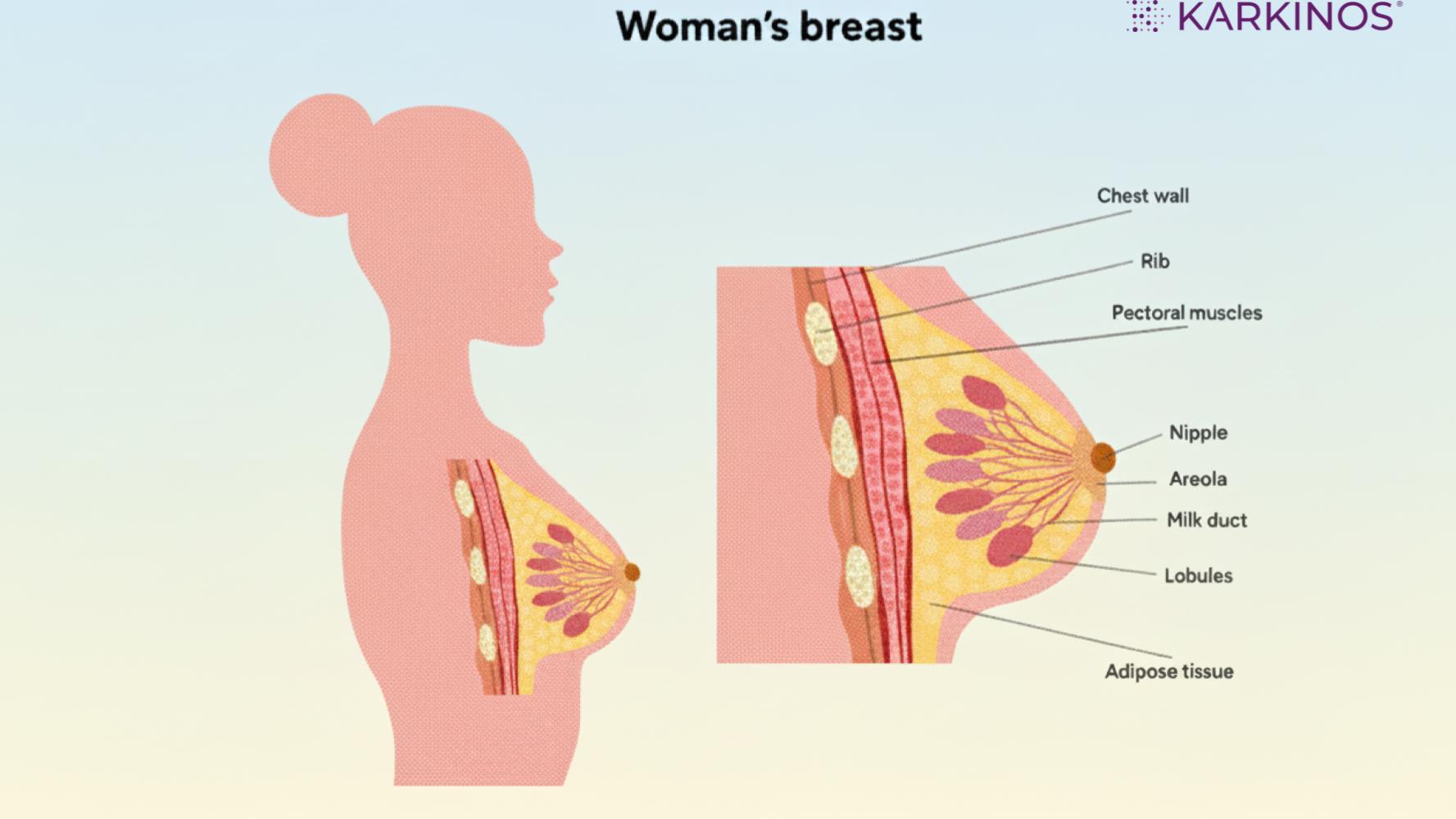
Fig 1: Structure of the breast
Lobes and Lobules
Each breast has 15 to 20 lobes arranged in a radial pattern around the nipple, similar to the spokes of a wheel. These lobes are further divided into smaller units called lobules.
The milk-producing units of the breast are the mammary alveoli, which are small, hollow sacs lined with specialised luminal epithelial cells that produce breast milk. These alveoli are covered by myoepithelial cells, which contract to push the milk out. When milk is secreted, it flows from the lumen of these sacs into the milk ducts.’
During lactation (nursing or breastfeeding), the synthesis of milk in these alveoli is regulated by the hormone prolactin.
**Cancer condition: Most breast cancers arise from the Terminal Ductal Lobular Unit (TDLU) — the junction between the smallest duct and its associated lobule. This is why understanding normal lobular anatomy is the true foundation of breast health literacy. **
The Ductal System
Each breast lobule is connected to a small duct that joins larger ducts, ultimately leading to a single main duct for each lobe, known as the lactiferous duct. In total, there are about 15 to 20 lactiferous ducts that come together at the nipple.
As they approach the nipple, they expand to create a small reservoir called the lactiferous sinus, where milk can collect. When a baby suckles, milk from these sinuses is released through the openings at the surface of the nipple during breastfeeding.
Stroma: The Supporting Framework
The glandular tissue of the breast is embedded within a supporting framework called the stroma, which consists of two components: fibrous connective tissue and fatty (adipose) tissue.
The fibrous tissue condenses into bands known as Cooper’s ligaments, which tether the breast to the overlying skin and the underlying pectoral fascia. These ligaments are what give the breast its shape and firmness.
Cancer condition: **When breast cancer invades Cooper’s ligaments and causes them to contract, the skin above puckers, wrinkles, or folds — a clinical sign known as skin dimpling.**
The fatty tissue, distributed between and around the lobes, largely determines the size and softness of the breast. The relative proportion of glandular to fatty tissue defines what clinicians call breast density — a concept with significant implications for imaging and cancer risk.
The Nipple and Areola
The nipple is a cylindrical or conical projection typically positioned at the level of the fourth intercostal space. It contains smooth muscle fibres arranged in circular and longitudinal patterns, which enable erection in response to stimulation and contraction during breastfeeding. The 15 to 20 lactiferous ducts open individually at the nipple tip. Notably, the nipple has no hair follicles, fat, or sweat glands.
The areola is the round, pigmented area around the nipple. It contains special glands called Montgomery’s glands. These glands produce an oily substance that helps lubricate and protect the nipple and areola during breastfeeding.
In Indian women, the areola usually has a medium colour, ranging from light to dark brown depending on their skin tone. It may also darken during pregnancy and breastfeeding, which is a normal response to hormonal changes.
Lymphatic Drainage: Why It Matters
The breast has many lymphatic vessels that help drain fluid and immune cells. This drainage is important to know, especially because breast cancer often spreads through these lymphatic channels.
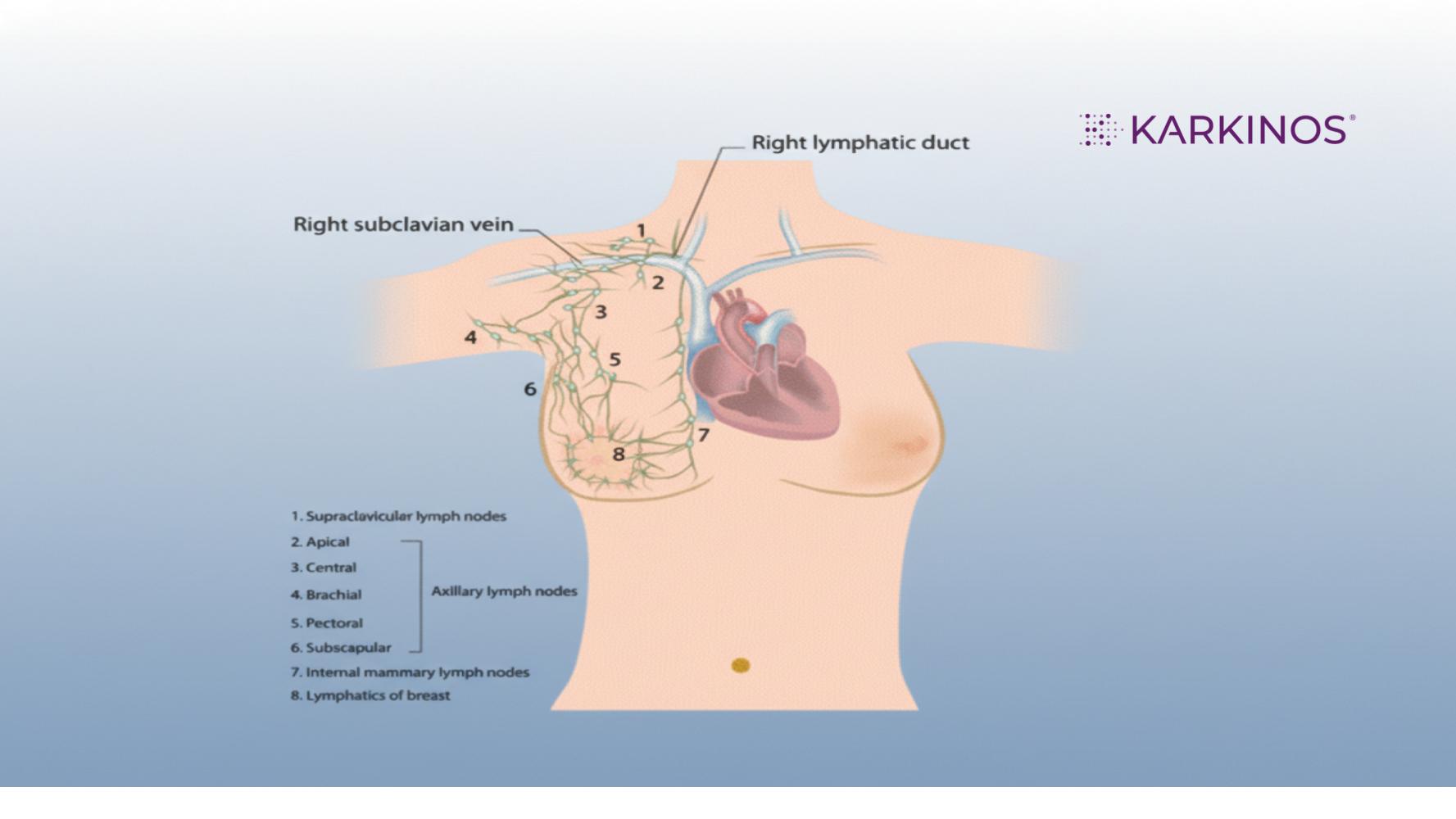
Fig 2: Representation of the lymphatic system of the breast
Lymph from the breast collects in a network called the subareolar plexus, located beneath the areola. From here, the drainage follows several pathways:
- Approximately 75% drains into the axillary (armpit) lymph nodes, which is why swollen, hard nodes in the armpit can be an early warning sign of breast cancer
- About 20% drains into the parasternal (internal mammary) nodes along the chest wall
- The remaining 5% drains upwards to the supraclavicular (above the collarbone) lymph nodes and to the intercostal lymph nodes near the ribs.
This anatomy explains why surgeons examine and remove axillary lymph nodes when treating breast cancer. These nodes act as the primary gatekeepers and, when cancer cells are present, signal the likelihood of wider spread.
Breast Physiology Across a Woman’s Lifetime
The breast undergoes transformation at every major hormonal milestone of a woman’s life.
Puberty: The First Awakening
Breast development (called thelarche) is usually the first sign of puberty in girls, typically beginning between ages 9 and 13 in Indian girls, though the range varies.
Rising oestrogen levels from the developing ovaries stimulate growth of the ductal system. The fat and connective tissue increase, giving the breast its characteristic shape. Full glandular development, however, does not occur until pregnancy.
During this phase, the areola enlarges and darkens, and the nipples become more prominent. Many girls experience breast tenderness, a normal response to the flood of hormonal activity.
The Reproductive Years: Cyclical Changes
During the reproductive years, breast tissue is very responsive to the hormonal changes in oestrogen and progesterone that occur throughout the menstrual cycle.
In the first half of the cycle (the follicular phase), rising oestrogen promotes ductal growth. After ovulation, progesterone stimulates the development of lobules in preparation for a potential pregnancy.
This is why many women experience breast fullness, heaviness, or tenderness in the days before menstruation, a phenomenon called cyclical mastalgia, which is entirely normal.
Pregnancy and Lactation: Maximum Development
Pregnancy triggers the most profound transformation of breast tissue. Under the combined influence of oestrogen, progesterone, prolactin, and human placental lactogen, the breast undergoes rapid growth. The ductal system branches extensively, lobules multiply, and secretory alveoli develop for the first time.
By mid-pregnancy, the breasts are anatomically prepared for milk production. However, actual lactation is suppressed until after delivery, when the fall in placental hormones allows prolactin to stimulate milk synthesis.
Colostrum (the thick, yellowish pre-milk rich in immune proteins and growth factors) may begin to leak from the nipples during the third trimester. After childbirth, milk letdown is triggered by the baby’s suckling via the hormone oxytocin, which causes the myoepithelial cells surrounding the alveoli to contract and expel milk into the ducts.
For Indian women, where breastfeeding rates remain high and extended breastfeeding is culturally common, understanding these physiological changes helps normalise the breast changes of pregnancy and lactation — and aids in recognising deviations from normal, such as mastitis or blocked ducts.
After Lactation: Involution
When breastfeeding ceases, the secretory alveoli shrink and gradually disappear in a process called involution. The breast never fully returns to its pre-pregnancy state — some permanent structural change remains, which is why multiparous (multiple-pregnancy) women often notice their breasts are softer and less firm than before. Some degree of ptosis (drooping) is a normal consequence of the ligamentous and skin stretching that occurs during pregnancy and lactation.
Perimenopause and Menopause: The Transition
As oestrogen levels begin their gradual decline in the perimenopausal years (typically the mid-40s for Indian women, though earlier menopausal onset has been observed in some Indian populations), the glandular breast tissue progressively involutes and is replaced by fatty tissue. The breasts may become softer, less dense, and more pendulous. Skin elasticity decreases, and Cooper’s ligaments may weaken, contributing to further ptosis.
After menopause, the breasts naturally contain more fat and less glandular tissue. This is helpful for screenings because fat appears dark on a mammogram. Since most tumours or abnormalities appear bright white, they stand out clearly against the dark background, making them much easier for doctors to find.
The Postmenopausal Years
In postmenopausal women, the breast typically undergoes atrophy (shrinkage) of the glandular tissue, leading to a generally smaller and softer appearance. Associated changes include nipples becoming less prominent and the areola potentially lightening in colour.
Despite these physical changes, the breast retains its essential functions and susceptibility: its lymphatic drainage pathways remain, it is still influenced by hormones (including exogenous ones like Hormone Replacement Therapy), and, crucially, the risk of malignant change persists and increases with advancing age.
What Makes Indian Women Distinctive
While breast anatomy is fundamentally similar across populations, there are population-specific features that have direct clinical relevance for Indian women.
Body Composition and Breast Volume
In India, women generally have a lower average Body Mass Index (BMI) compared to women in Western or Middle Eastern regions. Because breast size is closely linked to overall body fat, this lower BMI typically results in smaller average breast volumes among Indian women.
Historically, surgical guidelines and breast implant sizing charts were based on data from Western body types. As a result, these charts often do not fit the Indian context. To ensure safety and natural-looking results, medical professionals in India adapt these guidelines to better suit the specific physical proportions and smaller frames often found in the Indian population.
Breast Ptosis/Prolapse
Research on breast anthropometry in Indian women has consistently noted a greater degree of natural ptosis (drooping) compared to Western populations. This is reflected in measurements such as the sternal notch-to-nipple distance and the clavicle-to-nipple distance, which tend to be greater in Indian women than in those with larger breast volume. This is a normal anatomical variant, not a pathological finding, and should not cause unnecessary concern.
Breast Density in Indian Women
Breast density — the proportion of fibroglandular to fatty tissue — is an important factor in both cancer risk and mammographic interpretation. Studies from Indian institutions, including data from PGIMER Chandigarh, show that breast density in the Indian population is generally lower than in Western populations, with a larger proportion of Indian women having predominantly fatty breasts.
Breast density decreases with age in Indian women, as it does globally: younger women have denser breasts due to the predominance of glandular tissue, while postmenopausal women show greater fatty replacement. This has a significant implication: mammography tends to be more effective in older Indian women, whose lower-density breasts allow greater diagnostic clarity.
Dense breasts are not abnormal; approximately half of all women over 40 have dense breasts, but women with high breast density face a four- to six-fold increased risk of breast cancer compared to those with predominantly fatty breasts. This is because dense tissue can mask abnormalities on mammograms and may indicate a higher background of active glandular tissue.
Younger Age at Breast Cancer Diagnosis
One of the most important epidemiological distinctions for Indian women is the age profile of breast cancer. In India, a disproportionately high number of breast cancers are diagnosed in women under 40 compared to Western countries, where breast cancer is predominantly a disease of older women. This has implications for screening, awareness, and the age at which self-examination and clinical review should begin.
Recognising What is Normal
A thorough understanding of normal breast anatomy and its expected changes is the foundation of all breast health surveillance. Women who know their own breasts — their typical feel, their cyclical changes, their response to pregnancy and age — are far better equipped to notice when something has changed.
Normal variations that women should be aware of and not alarm themselves over include:
|
Changes that warrant prompt medical attention include a new lump or thickening, skin dimpling or puckering, new nipple inversion (in a nipple that was previously everted), nipple discharge (particularly if bloody or from one duct only), changes in skin texture (such as the orange-peel appearance of peau d’orange), and persistent unexplained pain.
Conclusion
Breast anatomy and physiology are dynamic; they represent a woman’s hormonal journey expressed through her tissue. For Indian women, understanding this journey is both empowering and crucial for health.
By learning about the structure of the breast and how it changes throughout puberty, pregnancy, and menopause, as well as recognising how Indian women’s breast anatomy may differ from what is described in Western textbooks, individuals can build a foundational knowledge for informed and proactive breast health.
This knowledge does not replace clinical care — but it makes that care possible. A woman who understands her own anatomy is one who will notice the change that matters, seek help when needed, and advocate for herself with confidence.
Disclaimer: This article is intended for educational purposes only and does not constitute medical advice. For personalised guidance, please consult a qualified healthcare professional.
References
India-Specific Studies
- Mokkapati PR, Gowda M, Deo S, et al. Breast Anthropometry — Results of a Prospective Study Among Indian Breast Cancer Patients. Indian Journal of Surgical Oncology. 2020;11(1):28–34. DOI: 10.1007/s13193-019-01031-3 | PMC: PMC7064648
- Anthropometric Breast Measurements in North Indian Women. Indian Journal of Surgery. 2021. DOI: 10.1007/s12262-021-03069-6
- Singh S, et al. Breast density in screening mammography in Indian population — Is it different from the western population? The Breast Journal. 2018. DOI: 10.1111/tbj.12949 | PubMed: 29139590
- Sudhir R, Sannapareddy K, et al. Clinico-radio-pathological Features and Biological Behavior of Breast Cancer in Young Indian Women. Indian Journal of Radiology & Imaging. 2021;31(2):323–332. DOI: 10.1055/s-0041-1734342 | PMC: PMC8448222
- Newton MV, et al. How “Breast Aware” are Indian Women? Annals of African Medicine. 2024;23(3):372–378. DOI: 10.4103/aam.aam_194_23 | PMC: PMC11364323
- Vishwakarma G, et al. Reproductive factors and breast cancer risk: a meta-analysis of case-control studies in Indian women. South Asian Journal of Cancer. 2019;8(2):80–84. DOI: 10.4103/sajc.sajc_317_18
Foundational Anatomy & Physiology References
- Pandya S, Moore RG. Breast development and anatomy. Clinical Obstetrics and Gynecology. 2011;54(1):91–95. DOI: 10.1097/GRF.0b013e318207ffe9 | PubMed: 21278507
- Functional anatomy and physiology of the female breast. Obstetrics and Gynecology Clinics of North America. 1994. PubMed: 7816404
- Johnson MC. Anatomy and Physiology of the Breast. In: Jatoi I, Kaufmann M (eds). Management of Breast Diseases. Springer, Berlin, Heidelberg. 2010. DOI: 10.1007/978-3-540-69743-5_1
10. Sabel MS. Anatomy and physiology of the breast. In: Essentials of Breast Surgery. Wiley Online Library. 2015. DOI: 10.1002/9781118655412.ch37
Karkinos Healthcare